Role of Diagnostic Laparoscopy in Abdominal Trauma
Prof Dr Anisur Rahman
Penetrating and blunt injury of the abdomen are common surgical admission in the emergency department. Most of these patients are poly trauma victims with multiple injuries involving several anatomical areas. Abdominal injury can be immediate life threatening due to bleeding and hypotension. Ultra sonogram and CT scan may point to the extent of blood loss and/or injury to solid organs. But at times the source of bleeding can be difficult to ascertain from CT scan.
Diagnostic Laparoscopy is a useful tool to determine the extent of injury and to detect the source of bleeding. Since minor injury to liver or spleen at times may be treated conservatively, Diagnostic Laparoscopy is an important step in avoiding a Laparotomy. This spares the patient from unnecessary Laparotomy with its associated morbidities.
The following case shows how a Diagnostic Laparoscopy helped in avoiding Laparotomy.
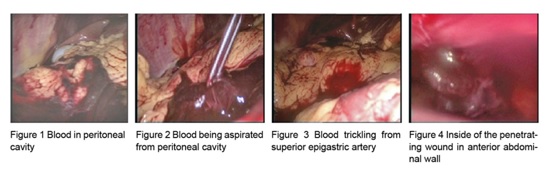
A 23 year old male patient was stabbed several times in the abdomen and came to Emergency Department from a rural area after about 5 hours from the time of incidence. On examination he had three sharp injuries on anterior abdominal wall, one of which in midline looked deep. He was semiconscious, tachypnic with a pulse of 130/min and BP of 90/60mm Hg with no history of passage of urine since the assault. The abdomen was distended and tense, bladder was empty and bowel sound was sluggish. Intravenous fluid and antibiotic was started on patient and blood bank was alerted. Urgent CT of abdomen reported large volume of fluid in abdominal cavity and no apparent injury to the solid organs or to the GI tract. Patient was shifted to OT with the plan to do Diagnostic Laparoscopy and Laparotomy if required. A 30 degree scope was introduced through umbilical port. There was huge volume of clotted and fluid blood in the peritoneal cavity which was aspirated out. Saline wash was given. No injury was seen in liver and spleen. Small gut was also normal. There was no apparent injury to the mesentery. Blood was seen spurting from the inner entry point of abdominal wall in midline. The other two stab injuries had not penetrated inside the peritoneal cavity. Obviously the superior epigastric artery was transected by the stab injury in midline and the patient had been bleeding inside the abdomen profusely. After adequate wash of the peritoneal cavity the scope was taken out and pneumoperitoneum was reversed. The midline injury was extended a little and the epigastric artery was ligated. The patient stabilized after two units of whole blood transfusion. The patient had uneventful recovery and was discharged from hospital two days later.
The case illustrates the importance of Diagnostic Laparoscopy in abdominal trauma. The patient was spared a conventional Laparotomy and he left the hospital with minimum morbidity. In case of Abdominal Trauma, the trauma surgeon in a hospital with laparoscopy setup should use Diagnostic Laparoscopy in conjunction with imaging technique to provide a better and safer alternative to Laparotomy.