Treatment of Segmental Fracture Shaft of Femur
Dr Aminul Hassan, Dr Masum Billah
Segmental fractures of long bones are prone to non union or delayed union because of devascularization of the segmental fragment at the time of injury (usually high velocity injury) or during internal fixation (due to soft tissue injury). Usually in this kind of fracture both the endosteal and periosteal blood supplies are interrupted during injury or surgical procedure. Most of these fractures need primary bone graft or bone graft later on. So it is advisable to try to preserve the blood supply of the segmental fracture during internal fixation.
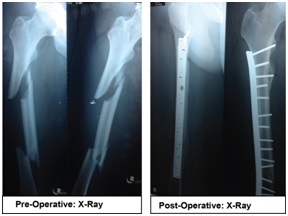 A 43 years old gentleman was admitted via Accident & Emergency department with history of road traffic accident followed by pain & swelling in right thigh & right hand with abrasion in multiple sites of body. On X-Ray comminuted segmental fracture of right femur with fracture of base of right 1st & 2nd metacarpal bone was seen.
A 43 years old gentleman was admitted via Accident & Emergency department with history of road traffic accident followed by pain & swelling in right thigh & right hand with abrasion in multiple sites of body. On X-Ray comminuted segmental fracture of right femur with fracture of base of right 1st & 2nd metacarpal bone was seen.
On examination there was tenderness, swelling & deformity of right femur with external rotation of right lower limb. Movement of right lower limb & right hand was painful & restricted, there was swelling of right palm over 1st metacarpal bone, multiple abrasions over forehead and no neurovascular deficit. He was able to move all toes of right foot and fingers of right hand actively. He was a known patient of hypertension, DM and S/P PTCA with stenting done on 2012. Initially patient was immobilized by skin traction on right lower limb with 2 kg weight and below elbow volar cast was given on right forearm. Other vital parameters were within normal limit.
 After proper evaluation and counseling with the patient and patient’s attendant about the fracture condition and outcome of treatment he underwent open reduction & internal fixation of right femur by plate & screws (16 holes broad DCP & 15 screws) under epidural anesthesia. His post operative period was uneventful. During his post operative hospital stay he took physiotherapy under direct supervision of surgeon and physiotherapist to improve the power of muscles and range of motion of all joints of right lower limb. He was on non weight bearing movement for twelve weeks and was on regular follow up periodically. He continued the muscle building exercise and active joint movement exercise at home regularly. Now he can stand without any supports and can walk independently, he is enjoying his daily life and performs his daily functional activities as before with confidence.
After proper evaluation and counseling with the patient and patient’s attendant about the fracture condition and outcome of treatment he underwent open reduction & internal fixation of right femur by plate & screws (16 holes broad DCP & 15 screws) under epidural anesthesia. His post operative period was uneventful. During his post operative hospital stay he took physiotherapy under direct supervision of surgeon and physiotherapist to improve the power of muscles and range of motion of all joints of right lower limb. He was on non weight bearing movement for twelve weeks and was on regular follow up periodically. He continued the muscle building exercise and active joint movement exercise at home regularly. Now he can stand without any supports and can walk independently, he is enjoying his daily life and performs his daily functional activities as before with confidence.
Proper operative management and fixation of long bone fracture may reduce the hospital stay and
patient can move freely without plaster cast or any support. It also significantly reduces the need for pain medications. Patient can go back to his workplace earlier with improved quality of life.