Prader Willi Syndrome, a rare genetic disorder
Dr Shahnaz Parvin Siddiqua, Dr Runa Laila, Dr Khorshed Alam, Dr Nargis Ara Begum
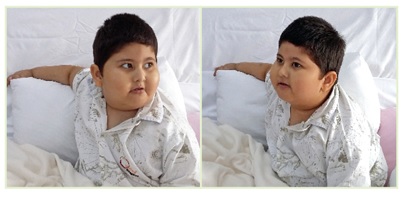
A 4½ years old male child was referred to United Hospital from BIRDEM with complaints of severe respiratory distress, generalized anasarca and severe respiratory acidosis; patient being in need of ventilator support. On examination the boy was dyspneic with severe chest indrawing, tachypneic, tachycardic, hypoxic in room air, hypotensive & had significantly severe crepitations in lungs, significant hepatomegaly. He was short (height <3rd centile) but obese (weight >97th centile). He had small hands and feet, narrow forehead, almond shaped eyes, central obesity & chryptorchidism (right side).
 The male child gave history of being born by LUCS (lower uterine caesarean section) at term due to less fetal movement. He was the only child of consanguineous parents. As per history after delivery he was hypotonic and developed feeding difficulty for which he needed Neonatal Intensive Care Unit {NICU} support and continued nasogastric tube feeding for 2 months. He had delayed demonstrated milestone of development, speech delay, low I/Q, hyperphagia, excessive weight gain, history of repeated respiratory infection and hyperactive airway disease which were suggestive of Prader Willi Syndrome (PWS).
The male child gave history of being born by LUCS (lower uterine caesarean section) at term due to less fetal movement. He was the only child of consanguineous parents. As per history after delivery he was hypotonic and developed feeding difficulty for which he needed Neonatal Intensive Care Unit {NICU} support and continued nasogastric tube feeding for 2 months. He had delayed demonstrated milestone of development, speech delay, low I/Q, hyperphagia, excessive weight gain, history of repeated respiratory infection and hyperactive airway disease which were suggestive of Prader Willi Syndrome (PWS).
Upon admission the boy had respiratory failure and severe respiratory acidosis (PH=6.9, PCO2=106). He was kept on ventilator support along with cardiotonic & other supportive therapy.
He was extubated after 15 days followed by BIPAP support which was also gradually withdrawn afterwards. Then he was discharged after 25 days of hospital stay as a case of Pneumonia with respiratory failure and heart failure with Prader Willi Syndrome. This male child is under regular monthly follow up at United Hospital and so far leading a normal life.
Prader Willi Syndrome is a genetic disorder due to loss of function of specific gene on chromosome 15. It affects approximately 1 in 10000 to 1 in 25000 newborn. There are more than 400000 people who live with PWS around the world. This complex genetic condition presents with severe hypotonia, feeding difficulties at birth, voracious appetite and obesity in infancy, short stature (responsive to growth hormone), small hand and feet, hypogonadism, intellectual disability, type 2 diabetes mellitus and delayed puberty. There is no specific treatment for PWS. Supportive treatment like behavioral modification therapy, developmental therapy, cognition stimulation and speech therapy, growth & sex hormone therapy are helpful. Newer medication like beloranib (analog of fumagillin) can play role in controlling appetite and obesity.