Missed Diagnosis of Meckel’s Diverticulum as a Cause of Recurrent Intestinal Obstruction Over 8 Years – Case Report
Prof Dr Anisur Rahman
Post operative intestinal obstruction is a known complication which can occur starting from immediate post operative period to many years later. But early intestinal obstruction due to a missed pathology during the initial surgery is not very common. Here we present such an uncommon case of post operative intestinal obstruction.
Patient, a 38 year old male, had open appendicectomy in 2006 in a district hospital. Since then he had recurrent attacks of intestinal obstruction for which he was admitted in different hospitals at home and abroad. During his last admission in hospital abroad, he was advised surgery. He preferred to return home to have the surgery.
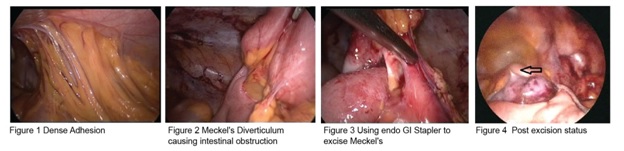
At Diagnostic Laparoscopy dense adhesions were seen in the region of appendix, which were divided and the intestine was freed. On further dissection the finding came out to be Meckel’s Diverticulum which was causing the intestinal obstruction due to a strong band extending from the tip to the abdominal wall compressing the intestine. The adhesions were divided and the Meckel’s Diverticulum was excised laparoscopically using endo GI stapler. The patient had an uneventful postoperative recovery.
Meckel’s Diverticulum is a congenital pouch on the wall of the distal ileum which occurs in approximately 2% of the population, of that only 2% are symptomatic and they tend to be typically below the age of two. This case is a unique one as the diagnosis is very unusual; Meckel’s Diverticulum being very rare in adults and is usually diagnosed at laparotomy. Most cases are treated by laparotomy and excision by wedge resection. This patient had suffered for 8 years because appropriate diagnosis was not made and the primary surgeon did not follow the dictum of examining the last 2 feet of terminal ileum during appendicectomy. This also shows the superiority of laparoscopic appendicectomy over open procedure, as overall evaluation of the other suspected pathologies can be made.